
CLINICAL TRIAL DESIGN SOFTWARE
Instructions: To access the software online click the red circle or the title. To download a desktop version, click the download arrow. To expand software description, mouse over the description.
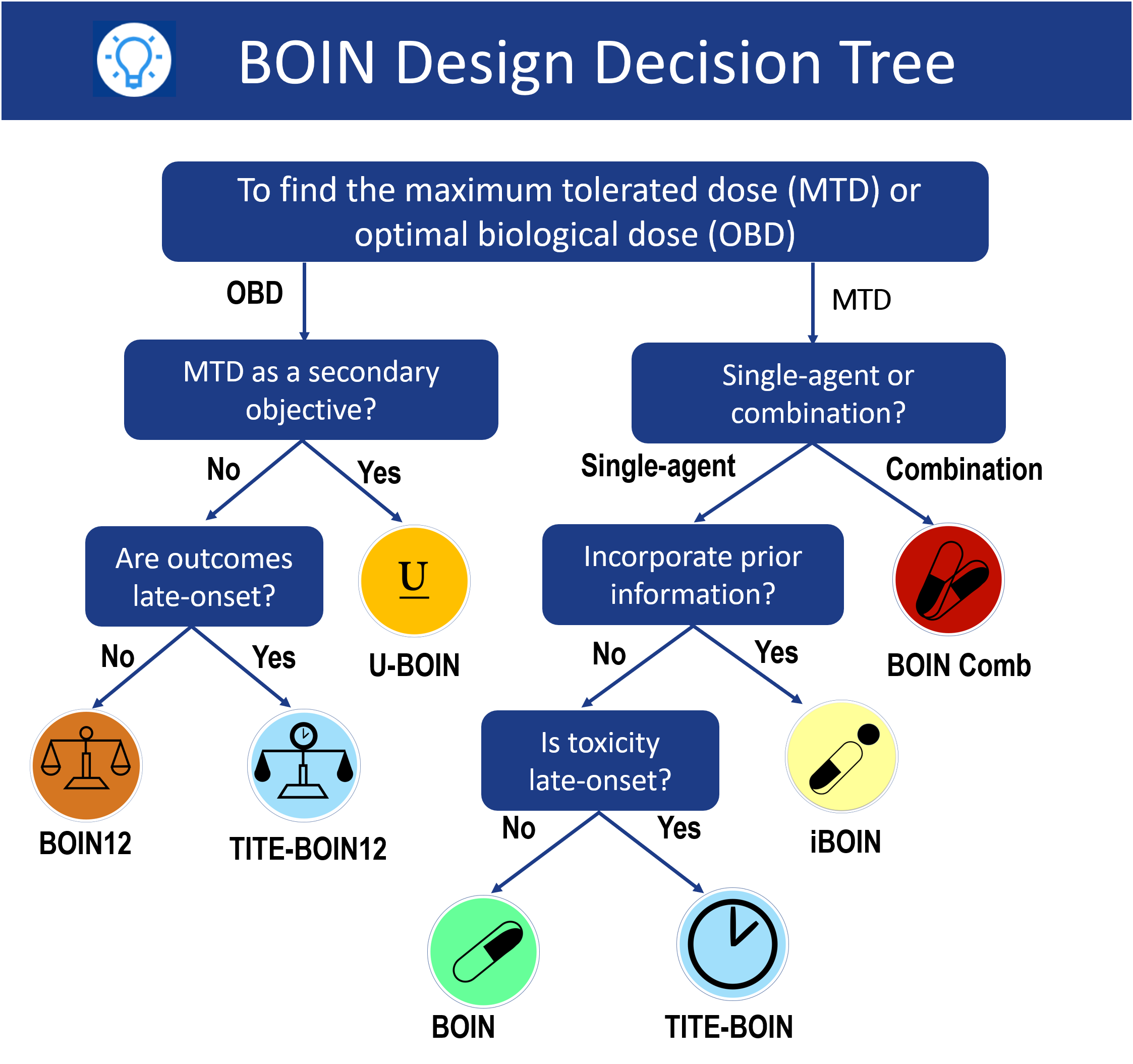
Find MTD for single-agent trials
BOIN
Use default non-informative prior (standard BOIN)
iBOIN
Use informative prior to incorporate historical data
To find optimal biological dose (OBD)
BOIN12
Both toxicity and efficacy are quickly ascertainable
TITE-BOIN12
Toxicity or/and efficacy take long time to be scored
To find backfill
BF-BOIN
Backfill Bayesian Optimal Interval Design for Phase I Clinical Trials
BARD
A two-stage dose optimization design integrating dose escalation, backfill, and adaptive randomization
How to choose a design?
QUALITY CONTROL
Our Software is developed according to industry standard for highest quality
- Source code has been reviewed by both software engineers and clinical trial experts for accuracy, completeness, repeatability, rigor, and robustness.
- Our software has been stress-tested extensively in edge cases that arose from real-world research.
- We receive feedback from experts worldwide, constantly update our software, and beta-test out it internally before publication.
- We leverage best-in-class tools such as Microsoft’s Visual Studio to ensure syntactical correctness and absence of simple errors.
- Every file is carefully maintained in Microsoft’s Team Foundation Server source control system to track and document modifications.
- We leverage proven technologies to produce reproducible, reliable, and stable applications.
MEET OUR TEAM
Our team includes Drs. Ying Yuan, J. Jack Lee, Suyu Liu, and Ruitao Lin, together with their current and former lab members. Our mission is to enhance the safety, efficacy, efficiency, and overall success of clinical research and drug development by developing and implementing innovative adaptive clinical trial designs.
Principal Investigators
Ying Yuan, Ph.D., Bettyann Asche Murray Distinguished Professor, University of Texas MD Anderson Cancer Center
- Bayesian adaptive clinical trial designs
- Statistical analysis of missing data
- Bayesian modeling and hypothesis testing
- Mediation analysis for behavioral and social research
J. Jack Lee, Ph.D., M.S., D.D.S., Professor, University of Texas MD Anderson Cancer Center
- Design and analysis of clinical trials
- Survival analysis
- Statistical computation/graphics
- Incorporation of multiple biomarkers and adaptive designs

Suyu Liu, Ph.D., Associate Professor, University of Texas MD Anderson Cancer Center
- Phase I/II dose-finding methods
- Statistical methods for delayed outcomes
- Biomarker-based and biomarker-enriched designs
- Biomarker discovery for early cancer detection

Ruitao Lin, Ph.D., Associate Professor, University of Texas MD Anderson Cancer Center
- Adaptive Clinical Trial Design and Decision Making
- Bayesian Modeling for Complex High-Dimensional Data
- Integration of AI/ML, Causal Inference, and Clinical Trial Methodology
- Digital Twin Technologies for Personalized Trial Simulation and Optimization
Acknowledgment
We sincerely thank the following colleagues for their invaluable contributions and collaboration: Fangrong Yan, Chunyan Cai, Tom Murray, Haitao Pan, Yong Zang, Nan Chen, Ying-Wei Kuo, Yiyi Chu, Rongji Mu, Heng Zhou, Yanhong Zhou, Liangcai Zhang, Juan Posadas, Yixuan Zhao, Kai Chen, Yujie Zhao, Peng Yang, Shuqi Wang, Feng Tian,. Their expertise, dedication, and support have been instrumental in advancing our research and fostering a highly collaborative environment.
SELECTED PUBLICATIONS
-
Book
bayesian designs for phase i–ii clinical trials
- first edition
- authors: ying yuan, hoang q. nguyen, and peter f. thall
- isbn-13: 978-1498709552
- chapman & hall/crc biostatistics series
bayesian adaptive methods for clinical trials
- first edition
- authors: scott m. berry, bradley p. carlin, j. jack lee, and peter muller
- isbn-13: 978-143982548
- chapman & hall/crc biostatistics serie, vol. 38s
-
Clinical Trial Design
- Jun, Yin. and Yuan, Y. (2020) Checkerboard: A Bayesian Efficacy and Toxicity Interval Design for Phase I/II Dose-finding Trials, Journal of Biopharmaceutical Statistics, in press.
- Jin IH, Zhang Z, Yuan, Y. (2020) Social Network Mediation Analysis: a Latent Space Approach, Psychometrika, in press.
- Zhou, Y., Li, R., Kuo, Y., Lee, JJ. and Yuan, Y. (2020) BOIN Suite: a software platform to design and implement novel early phase clinical trials, JCO Clinical Cancer Informatics, to appear.
- Zhou, Y., Li, R., Yan, F., Lee, JJ. and Yuan, Y. (2020) A comparative study of Bayesian optimal interval (BOIN) design with interval 3+3 (i3+3) design for phase I oncology dose-finding trials, Statistics in Biopharmaceutical Research , in press.
- Lin, R., Yan, F., Li, D. and Yuan, Y. (2020) BOIN12: Bayesian Optimal Interval Phase I/II Trial Design for Utility-Based Dose Finding in Immunotherapy and Targeted Therapies, JCO precision oncology , to appear.
- Lin, R., Yin, G., Yuan, Y., and Yang, Z. (2020) Sample size re-estimation in adaptive enrichment design, Contemporary Clinical Trials, to appear.
- Lin, R.*, Thall, P., and Yuan, Y. (2020) BAGS: A Bayesian Group Sequential Clinical Trial Design with Adaptive Subgroup-Specific Survival Time Comparisons, Journal of the American Statistical Association , in press.
- Li, Y., Yuan, Y. (2020) PA-CRM: A Continuous Reassessment Method for Pediatric Phase I Oncology Trials with Concurrent Adult Trials, Biometrics, to appear.
- Pan, H., Cheng, C. and Yuan, Y. (2020) Bayesian adaptive linearization method for phase I drug combination trials with dimension reduction, Pharmaceutical Statistics, in press.
- Lin, R., Thall, P. and Yuan, Y. (2020) A Phase III Basket Trial Design to Optimize Dose-Schedule Regimes Based on Delayed Outcomes, Bayesian Analysis, in press.
- Pan, H., Lin, R., Zhou, Y. and Yuan, Y. (2020) Keyboard Design for Phase I Drug-Combination Trials, Contemporary Clinical Trials, 92:105972.
- Zho,u H., Chen, C., Sun, L. and Yuan, Y. (2020) Bayesian Optimal Phase II Clinical Trial Design with Time-to-event endpoint, Pharmaceutical Statistics, 19, 776-786.
- Han, Y., Yuan, Y., Cao, S., Li, M. and Zang, Y. (2020) On the Use of Marker Strategy Design to Detect Predictive Marker E.ect in Cancer Immunotherapy, Statistics in Biosciences, 12, 180195.
- Lin, R.*, Yuan, Y. and Thall, P. (2020) An Adaptive Trial Design to Optimize DoseSchedule Regimes with Delayed Outcomes, Biometrics, 76(1):304-315.
- Lin, R.*, Coleman R. and Yuan, Y. (2020) TOP: Time-to-Event Bayesian Optimal Phase II Trial Design for Cancer Immunotherapy, Journal of the National Cancer Institute, 112(1):38-45.
- Lin, R.* and Yuan, Y. (2020) Time-to-Event Model-Assisted Designs for Dose-Finding Trials with Delayed Toxicity, Biostatistics, 21(4):807-824.
- Yan F., Pan H., Zhang L., Liu S. and Yuan, Y. (2020) BOIN: An R Package for Designing Single- Agent and Drug-Combination Dose-Finding Trials Using Bayesian Optimal Interval Designs, Journal of Statistical Software , 94(13):1-32. doi:10.18637/jss.v094.i13.
- Lee JJ , Yin G. (2020) Principles and Reporting of Bayesian Trials, Journal of Thoracic Oncology, https://doi.org/10.1016/j.jtho.2020.10.010.
- Xu G, Zhu H, Lee JJ . (2020) Borrowing Strength and Borrowing Index for Bayesian Hierarchical Models. Comput Stat Data Anal 144, 4/2020. PMCID: PMC7185234.
- Chen N, Lee JJ . (2020) Bayesian cluster hierarchical model for subgroup borrowing in the design and analysis of basket trials with binary endpoints. Stat Methods Med Res : 2020 Sep;29(9):2717-2732. PMID: 32178585.
- Yuan Y, Lee JJ , Hilsenbeck SG. (2019) Model-Assisted Designs for Early-Phase Clinical Trials: Simplicity Meets Superiority. JCO Precision Oncology 3:1-12.
- Ruberg, SJ, Harrell, FE, Jr., Gamalo-Siebers, M., LaVange, L., Lee, JJ, Price, K., Peck, C. (2019) Inference and Decision Making for 21st-Century Drug Development and Approval. American Statistician 73(sup1):319-327.
- Chen N, Lee JJ. (2019) Bayesian hierarchical classification and information sharing for clinical trials with subgroups and binary outcomes. Biom J 61(5):1219-1231, 2019. PMID: 30506747.
- Zhou Y, Lee JJ and Yuan Y. (2019) A utility-based Bayesian optimal interval (U-BOIN) phase I/II design to identify the optimal biological dose for targeted and immune therapies. Stat Med 38(28):5299-5316, 12/2019. e-Pub 10/2019. PMID: 31621952.
- Zhu H, Piao J, Lee JJ , Hu F, Zhang L. (2019) Response adaptive randomization procedures in seamless phase II/III clinical trials. J Biopharm Stat 30(1):3-17. e-Pub 8/2019. PMID: 31454295.
- Slack, R.S., Peng, A., Chen, M., Liu, D., Yuan, Y. and Lee J.J. (2019) Bayesian Clinical Trials at the University of Texas MD Anderson Cancer Center: An Update, Clinical Trials, 16(6):645-656, PMID: 31450957.
- Yan, F., Thall, P. and Yuan, Y. (2019) One-Year Outcomes after PCI Strategies in Cardiogenic Shock, The New England Journal of Medicine, 380:1876-1877.
- Lin R.* and Yuan, Y. (2019) On the Relative Efficiency of Model-Assisted Designs: A Conditional Approach, Journal of Biopharmaceutical Statistics, 29(4):648-662.
- Huang J.*, Yuan, Y. and Wetter D. (2019) Latent Class Dynamic Mediation Model with Application to Smoking Cessation Data, Psychometrika, 84(1):1-18.
- Tang, R., Shen, J. and Yuan, Y. (2019) ComPAS: A Bayesian Drug-Combination Platform Design with Adaptive Shrinkage, Statistis in Medicine, 38(7):1120-1134.
- Ursino, M., Yuan, Y., Comets, E., Favrais, G., Friede, T., Lentz, F., Stallard, N., Zohar, S. (2019) A dose-finding design for seizure reduction in neonates. Journal of the Royal Statistical Society: Series C , 68 (2):427-444.
- Shin, S.*, Yuan, Y., Strong, L.C., Bojadzieva, J. and Wang, W. (2019) Bayesian Semiparametric Estimation of Cancer-specific Age-at-onset Penetrance with Application to Li-Fraumeni Syndrome. Journal of the American Statistical Association, 114(526):541-552.
- Ahn, J.*, Morita, S.,Wang W. and Yuan, Y. (2019) Bayesian Shared Parameter Models for Dyadic Longitudinal Data with Informative Missing Data. Statistical Methods in Medical Research , 28(1):70- 83.
- Hobbs BP, Chen N, Lee JJ. (2018) Controlled multi-arm platform design using predictive probability. Stat Methods Med Res 27(1):65-78. e-Pub 1/2016. PMCID: PMC5039108.
- Du Y, Cook JD, Lee JJ. (2018) Comparing three regularization methods to avoid extreme allocation probability in response-adaptive randomization. J Biopharm Stat. 28(2):1-11, e-Pub 3/2017. PMID: 28323532.
- Yin, G., Chen, N. and Lee, JJ. (2018) Bayesian Adaptive Randomization and Trial Monitoring with Predictive Probability for Time-to-Event Endpoint. Statistics in Biosciences 10(2):420-438.
- Mu, R., Yuan, Y., Xu, J. , Mandrekar, SJ., and Jun Y. (2019) gBOIN: A unified phase I trial design accounting for toxicity grades. Journal of the Royal Statistical Society: Series C, 68, 289-308.
- Pan, H*., Liu, S., Miao, D. and Yuan, Y. (2018) Sample size determination for mediation analysis of longitudinal data. BMC Medical Research Methodology, 18(1):32. doi: 10.1186/s12874-018-0473-2.
- Guo, B., Li, D. and Yuan, Y. (2018) SPIRIT: A Seamless Phase I/II Randomized Design for Immunotherapy Trials. Pharmaceutical Statistics, 17, 527-540.
- Zhou, H.*, Yuan, Y., and Nie, L. (2018) Accuracy, Safety and Reliability of Novel Phase I Trial Designs. Clinical Cancer Research, 24, 4357-4364.
- Yuan, Y., Lin, R., Li, D., Nie, L., and Warren K. (2018) Time-to-event Bayesian Optimal Interval Design to Accelerate Phase I Trials. Clinical Cancer Research, 24, 4921-4930.
- Zhou, H.*, Murray, T., Pan, H. and Yuan, Y. (2018) Comparative review of novel model-assisted designs for phase I clinical trials. Statistics in Medicine, 37, 2208-2222.
- Yan, F. Thall, PF., Lu, KH., Gilbert, MR., and Yuan, Y. (2018) Phase I-II clinical trial design: A state-of-the-art paradigm for dose finding, Annals of Oncology, 29, 694-699.
- Chu, Y.* and Yuan, Y. (2018) BLAST: Bayesian Latent Subgroup Design for Basket Trials Accounting for Patient Heterogeneity, Journal of the Royal Statistical Society: Series C, 67, 723-740.
- Murray, T., Yuan, Y., Thall, P., Elizondo, JH and Hofstetter, WL (2018) A Bayesian Utility-Based Stratified Medicine Design for the Effectiveness of Nutritional Prehabilitation in Thoracic Surgery, Biometrics, 74, 1095-1103.
- Chu, Y.* and Yuan, Y. (2018) A Bayesian Basket Trial Design Using Calibrated Bayesian Hierarchical Model. Clinical Trials, 15, 149-158.
- Shen, W*., Ning, J., Yuan, Y., Lok, A., Feng, Z. (2018) Model-free scoring system for risk prediction with application to hepatocellular carcinoma study, Biometrics, 74, 239-248.
- Liu, S., Guo, B. and Yuan, Y. (2018) A Bayesian Phase I/II Design for Immunotherapy Trials. Journal of the American Statistical Association, 113, 1016-1027.
- Murray, T.*, Thall, P. and Yuan, Y. (2018) A Bayesian Machine Learning Method for Optimizing Dynamic Treatment Regimes. Journal of the American Statistical Association, 113, 1255-1267.
- Riviere, M.K.*, Yuan, Y., Jourdan, J.H., Dubois, F. and Zohar, S. (2018) Phase I/II Dose-Finding Design for Molecularly Targeted Agent: Plateau Determination using Adaptive Randomization. Statistical Methods in Medical Research, 27, 466-479.
- Cai, C., Rahbar, M., Hossain, M., Yuan, Y. and Gonzales, N. (2017) A placebo-controlled Bayesian dose finding design based on continuous reassessment method in stroke research. Contemporary Clinical Trials Communications , 7:11-17.
- Yan, F., Mandrekar, SJ. and Yuan, Y. (2017) Keyboard: A Novel Bayesian Toxicity Probability Interval Design for Phase I Clinical Trials. Clinical Cancer Research, 23, 3994-4003.
- Chen, Z. , Li, Z, Zhuang, R., Yuan, Y., Kutner, M., Owonikoko, T., Curran, W. and Kowalski, J. (2017) Adaptive estimation of personalized maximum tolerated dose in cancer phase I clinical trials based on all toxicities and individual genomic profile, PLOS ONE, 12(1): e0170187.
- Guo, B. and Yuan, Y. (2017) Bayesian Phase I/II Biomarker-based Dose Finding for Precision Medicine with Molecularly Targeted Agents. Journal of the American Statistical Association , 112 , 508-520. ( Featured as JASA Applications and Case Studies – Invited Papers for 2018 JSM in Vancouver )
- Zhou, H.*, Lee, J. and Yuan, Y. (2017) BOP2: Bayesian Optimal Design for Phase II Clinical Trials with Simple and Complex Endpoints. Statistics in Medicine, 36, 3302-3314.
- Pan, H.* and Yuan, Y. (2017) A Calibrated Power Prior Approach to Borrow Information from Historical Data with Application to Biosimilar Clinical Trials. Journal of the Royal Statistical Society: Series C , 66, 979-996.
- Zang, Y.* and Yuan, Y. (2017) Optimal Sequential Enrichment Designs for Phase II Clinical Trials. Statistics in Medicine, 36, 54-66.
- Chu, Y.* and Yuan, Y. (2017) BLAST: Bayesian Latent Subgroup Design for Basket Trials Accounting for Patient Heterogeneity. Journal of the Royal Statistical Society: Series C , to appear.
- Chu, Y.* and Yuan, Y. (2017) A Bayesian Basket Trial Design Using Calibrated Bayesian Hierarchical Model. Clinical Trials, to appear.
- Liu, S., Guo, B. and Yuan, Y. (2017) A Bayesian Phase I/II Design for Immunotherapy Trials. Journal of the American Statistical Association , to appear.
- Murray, T.*, Yuan, Y. and Thall, P. (2017) A Bayesian Machine Learning Method for Optimizing Dynamic Treatment Regimes. Journal of the American Statistical Association , to appear.
- Yan, F., Mandrekar, SJ. and Yuan, Y. (2017) Keyboard: A Novel Bayesian Toxicity Probability Interval Design for Phase I Clinical Trials. Clinical Cancer Research, 23, 3994-4003.
- Zhou, H.*, Lee, JJ. and Yuan, Y. (2017) BOP2: Bayesian Optimal Design for Phase II Clinical Trials with Simple and Complex Endpoints. Statistics in Medicine , 36, 3302-3314.
- Pan, H.* and Yuan, Y. (2017) A Calibrated Power Prior Approach to Borrow Information from Historical Data with Application to Biosimilar Clinical Trials. Journal of the Royal Statistical Society: Series C , 66, 979-996.
- Guo, B.* and Yuan, Y. (2017) Bayesian Phase I/II Biomarker-based Dose Finding for Precision Medicine with Molecularly Targeted Agents. Journal of the American Statistical Association , 112, 508-520.
- Murray, T.*, Thall, P., Yuan, Y., McAvoy, S. and Gomez, D. (2017) Robust treatment comparison based on utilities of semi-competing risks in non-small-cell lung cancer. Journal of the American Statistical Association , 112, 11-23. ( Featured as JASA Applications and Case Studies – Invited Papers for 2018 JSM in Vancouver )
- Zang, Y.* and Yuan, Y. (2017) Optimal Sequential Enrichment Designs for Phase II Clinical Trials. Statistics in Medicine , 36, 54-66.
- Yuan, Y., Hess, K., Hilsenbeck, S. and Gilbert, M. (2016) Bayesian Optimal Interval Design: A Simple and Well-Performing Design for Phase I Oncology Trials. Clinical Cancer Research, 22, 4291-430.
- Yuan, Y., Guo, B, Munsell, M., Lu, K. and Jazzari, A. (2016) MIDAS: a practical Bayesian design for platform trials with molecularly targeted agents. Statistics in Medicine, 35, 3892-3906.
- Zang, Y.*, Liu, S. and Yuan, Y. (2016) Optimal Marker-strategy Clinical Trial Design to Detect Predictive Markers for Targeted Therapy. Biostatistics, 17, 549-560.
- Zhang, L.* and Yuan, Y. (2016) A Practical Bayesian Design to Identify the Maximum Tolerated Dose Contour for Drug Combination Trials. Statistics in Medicine, 35, 4924-4936.
- Riviere, M.K.*, Yuan, Y., Jourdan, J.H., Dubois, F. and Zohar, S. (2016) Phase I/II Dose-Finding Design for Molecularly Targeted Agent: Plateau Determination using Adaptive Randomization. Statistical Methods in Medical Research , to appear
- Chu, Y.*, Pan, H. and Yuan, Y. (2016) Adaptive dose modification for phase I clinical trials. Statistics in Medicine , 35, 3497-508.
- Iasonos, A. , Wages N., Conaway, M., Cheung, K., Yuan, Y. and O�Quigley, J. (2016) Dimension of Model Parameter Space and Operating Characteristics in Adaptive Dose-Finding Studies. Statistics in Medicine , 35, 3760-3775.
- Pan, H.* and Yuan, Y. (2016) A Default Method to Specify Skeletons for Bayesian Model Averaging Continual Reassessment Method for Phase I Clinical Trials. Statistics in Medicine, 36, 266-279.
- Zang, Y.*, J. Lee and Yuan, Y. (2016) Two-stage marker-stratified clinical trial design in the presence of biomarker misclassification. Journal of the Royal Statistical Society: Series C , 65, 585-601.
- Guo, B., Li, Y. and Yuan, Y. (2016) A dose-schedule-finding design for phase I/II clinical trials. Journal of the Royal Statistical Society: Series C , 65, 259-272.
- Chen, Z., Yuan, Y., Li, Z., Kutner, M., Owonikoko, T., Curran, W, Khuri, F. and Kowalski, J. (2015) Dose escalation with over-dose and under-dose controls in phase I/II clinical trials. Contemporary Clinical Trials , 43, 133-141.
- Shen, W.*, Ning, J. and Yuan, Y. (2015) Bayesian sequential monitoring design for clinical trials with non-compliance Statistics in Medicine , 34, 2104-2115.
- Zang, Y.*, Liu, S. and Yuan, Y. (2015) Optimal Marker-Adaptive Designs for Targeted Therapy Based on Imperfectly Measured Biomarkers. Journal of the Royal Statistical Society: Series C , 64, 635-650.
- Liu, S. and Yuan, Y. (2015) Bayesian Optimal Interval Designs for Phase I Clinical Trials. Journal of the Royal Statistical Society: Series C , 64, 507-523.
- Guo, B. and Yuan, Y. (2015) A Bayesian Design for Phase I/II Clinical Trials with Nonignorable Dropout. Statistics in Medicine , 34, 1721-1732.
- Shen, W.*, Ning, J. and Yuan, Y. (2015) A Direct Method to Evaluate the Time-dependent Predictive Accuracy for Biomarkers. Biometrics , 71, 439-449.
- Liu, S., Pan, H., Huang Q., Xia, J. and Yuan, Y. (2015) Bridging Continual Reassessment Method for Phase I Clinical Trials in Different Ethnic Populations. Statistics in Medicine, 10, 1681-1694.
- Riviere, M.K.*, Yuan, Y., Dubois, F. and Zohar, S. (2015) A Bayesian Dose-finding Design for Clinical Trials Combining a Cytotoxic Agent with a Molecularly Targeted Agent. Journal of the Royal Statistical Society: Series C , 64, 215-229.
- Jin, I.H.*, Liu, S., Thall, P. and Yuan, Y. (2014) Using Data Augmentation to Facilitate Conduct of Phase I/II Clinical Trials with Delayed Outcomes. Journal of the American Statistical Association , 109, 525-536.
- Riviere M.K., Yuan Y. , Dubois F. and Zohar S. (2014) A Bayesian dose-finding design for drug combination clinical trials based on the logistic model. Pharmaceutial Statistics, 13, 247-257.
- Zang, Y.*, Lee J. and Yuan, Y. (2014) Adaptive designs for identifying optimal biological dose for molecularly targeted agents. Clinical Trials, 11, 319-327.
- Cai, C.*, Liu, S. and Yuan, Y. (2014) A Bayesian Design for Phase II Clinical Trials with Delayed Responses Based on Multiple Imputation. Statistics in Medicine, 33, 4017-4028.
- Liu, S., Yuan, Y. , Castillo, R., Guerrero, T. and Johnson, V.E. (2014) Evaluation of Deformable Image Registration Spatial Accuracy Using a Bayesian Hierarchical Model. Biometrics, 70, 366-377.
- Cai, C.*, Yuan, Y. and Ji, Y. (2014) A Bayesian Phase I/II Design for Oncology Clinical Trials of Combining Biological Agents. Journal of the Royal Statistical Society: Series C , 63, 159-173.
- Liu, S., Yin, G. and Yuan, Y. (2013) Bayesian Data Augmentation Dose Finding with Continual Reassessment Method and Delayed Toxicity. Annals of Applied Statistics, 4, 2138-2156.
- Ahn, J.*, Yuan, Y., Parmigiani, G., Suraokar, M. B., Diao, L., Wistuba, I. and Wang W. (2013) DeMix: Deconvolution for mixed cancer transcriptomes using raw measured data. Bioinformatics, 29, 1865-1871.
- Cai, C.*, Yuan, Y. and Johnson, V.E. (2013) Bayesian adaptive phase II screening design for combination trials. Clinical Trials , 10, 353-362.
- Jin, I.H.*, Yuan, Y. and Liang, F. (2013) Bayesian analysis for exponential random graph models using the adaptive exchange sampler. Statistics and Its Interface, 6, 559-576.
- Zang, Y*. and Yuan, Y. (2013) A Shrinkage Method for Testing the Hardy-Weinberg Equilibrium in Case-Control Studies. Genetic Epidemiology , 37, 743-750.
- Yuan, Y., Thall, P. andWolf, J. (2012) Estimating Progression-free Survival When the Progression Status of Some Subjects is Unknown. Journal of the Royal Statistical Society: Series C , 61, 135-149.
- Yuan, Y. and Johnson, V.E. (2012) Goodness-of-Fit Diagnostics for Bayesian Hierarchical Models. Biometrics 68, 156-164.
- Huo, L.*, Yuan, Y. and Yin, G. (2012) Dose Finding in Drug Combinations with Discrete and Continuous Doses. Bayesian Analysis , 7, 235-252.
- Yuan, Y. and Yin, G. (2011) Robust EM Continual Reassessment Method in Oncology Dose Finding. Journal of the American Statistical Association 106, 818-831. ( featured article )
- Lei, X., Yuan, Y. and Yin, G. (2011) Bayesian phase II adaptive randomization by jointly modeling time-to-event efficacy and binary toxicity. Lifetime Data Analysis 17, 156-174.
- Yuan, Y. and Yin, G. (2011) Bayesian phase I/II drug-combination trial design in oncology. Annals of Applied Statistics , 5, 924-942.
- Yuan, Y. and Yin, G. (2011) Bayesian Hybrid Design in Phase I Oncology Clinical Trials. Statistics in Medicine, 30, 2098-2108.
- Yuan, Y., Huang, X. and Liu, S. (2011) A Bayesian response-adaptive covariate-balanced randomization design for clinical trials. Statistics in Medicine , 30, 1218-1229.
- Yuan, Y. and Yin, G. (2011) On adaptive randomization: is it useful? Journal of Clinical Oncology, 29, e390-e392
- Yin, G., Ma, Y., Liang, F. and Yuan, Y. (2011) Stochastic generalized method of moments. Journal of Computational and Graphical Statistics 20, 714-727.
- Yuan, Y. and Yin, G. (2011) Dose-response curve estimation: A semiparametric mixture approach. Biometrics 67, 1543-1554.
- Yin, G. and Yuan, Y. (2009) Bayesian Model Averaging Continual Reassessment Method in Phase I Clinical Trials. Journal of the American Statistical Association 104, 954-968.
- Song P.X., Li, M. and Yuan, Y. (2009) Joint Regression Analysis of Correlated Data Using Gaussian Copulas. Biometrics 65, 60-68.
- Yin, G. and Yuan, Y. (2009) A latent contingency table approach to dose-finding for combinations of two agents. Biometrics 65, 866-875.
- Yin, G. and Yuan, Y. (2009) Bayesian Dose-finding in Oncology for Drug Combinations by Copula Regression. Journal of the Royal Statistical Society: Series C 58, 211-224.
- Yuan, Y. and Yin, G. (2009) Bayesian Dose-finding by Jointly Modeling Toxicity and Efficacy as Time-to-Event Outcomes. Journal of the Royal Statistical Society: Series C 58, 719-736.
- Yuan, Y. and Johnson, V.E. (2008) Bayesian Hypothesis Tests Using Nonparametric Statistics. Statistica Sinica 18, 1185-1200
- Yuan, Y. and Yin, G. (2008) Sequential Continual Reassessment Method for Two-dimensional Dose Finding. Statistics in Medicine 27, 5664-5678.
- Lee JJ, Liu DD. A predictive probability design for phase II cancer clinical trials. Clin Trials 5(2):93-106, 2008. PMID: 18375647.
- Zhou X, Liu S, Kim ES, Herbst RS, Lee JJ. Bayesian adaptive design for targeted therapy development in lung cancer--a step toward personalized medicine. Clin Trials 5(3):181-93, 2008. PMID: 18559407.
- Le Tourneau C, Lee JJ, Siu LL. Dose escalation methods in phase I cancer clinical trials. J Natl Cancer Inst 101(10):708-20, 5/2009. e-Pub 5/2009. PMCID: PMC2684552.
- Biswas S, Liu DD, Lee JJ, Berry DA. Bayesian clinical trials at the University of Texas MD Anderson Cancer Center. Clin Trials 6(3):205-16, 6/2009. PMCID: PMC2913209.
- Cao J, Lee JJ, Alber S. Comparison of Bayesian sample size criteria: ACC, ALC, and WOC. J Stat Plan Inference 139(12):4111-4122, 12/2009. PMCID: PMC4279958.
- Lee JJ, Xuemin Gu , Suyu Liu. Bayesian adaptive randomization designs for targeted agent development. Clin Trials 7(5):584-96, 10/2010. e-Pub 6/2010. PMCID: PMC5110207.
- Gu X, Lee JJ. A simulation study for comparing testing statistics in response-adaptive randomization. BMC Med Res Methodol 10(48):48, 2010. e-Pub 6/2010. PMCID: PMC2911470.
- Lee JJ. Demystify statistical significance--time to move on from the p value to bayesian analysis. J Natl Cancer Inst 103(1):2-3, 1/2011. e-Pub 12/2010. PMID: 21131578.
- Yin G, Chen N, Lee JJ. Phase II trial design with Bayesian adaptive randomization and predictive probability. J R Stat Soc Ser C Appl Stat 61(2):219-35, 3/2012. PMCID: PMC3832255.
- Lee JJ, Chen N, Yin G. Worth adapting? Revisiting the usefulness of outcome-adaptive randomization. Clin Cancer Res 18(17):4498-507, 9/2012. e-Pub 7/2012. PMCID: PMC3495976.
- Lee JJ, Chu CT. Bayesian clinical trials in action. Stat Med 31(25):2955-72, 11/2012. e-Pub 6/2012. PMCID: PMC3495977.
- Jiang F, Lee JJ, Müller P. A Bayesian decision-theoretic sequential response-adaptive randomization design. Stat Med 32(12):1975-1994, 5/2013. e-Pub 1/2013. PMCID: PMC3873748.
- Chen N, Lee JJ. Optimal continuous-monitoring design of single-arm phase ii trial based on the simulated annealing method. Contemp Clin Trials 35(1):170-178, 5/2013. e-Pub 3/2013. PMCID: PMC3741066.
- Yao JC, Meric-Bernstam F, Lee JJ, Eckhardt SG. Accelerated approval and breakthrough therapy designation: oncology drug development on speed? Clin Cancer Res 19(16):4305-4308, 8/2013. e-Pub 7/2013. PMCID: PMC4167364.
- Gu X, Yin G, Lee JJ. Bayesian two-step Lasso strategy for biomarker selection in personalized medicine development for time-to-event endpoints. Contemp Clin Trials 36(2):642-50, 11/2013. e-Pub 9/2013. PMCID: PMC3873734.
- Kim MO, Liu C, Hu F, Lee JJ. Outcome-adaptive randomization for a delayed outcome with a short-term predictor: imputation-based designs. Stat Med 33(23):4029-42, 10/2014. e-Pub 5/2014. PMCID: PMC4159410.
- Zang Y, Lee JJ. Adaptive clinical trial designs in oncology. Chin Clin Oncol 3(4):49, 12/2014. PMID: 25841530.
- Marchenko, O., Fedorov, V., Lee, J.J., Nolan, C., Pinheiro, J. Adaptive Clinical Trials: Overview of Early-Phase Designs and Challenges. Therapeutic Innovation and Regulatory Science 48(1):20-30, 2014.
- Alber, S. A., Lee, J. J. Calibrating the prior distribution for a normal model with conjugate prior. Journal of Statistical Computation and Simulation:1-21, 2014.
- Du Y, Wang X, Lee JJ. Simulation study for evaluating the performance of response-adaptive randomization. Contemp Clin Trials 40:15-25, 1/2015. e-Pub 11/2014. PMCID: PMC4314433.
- Liu S, Lee JJ. An overview of the design and conduct of the BATTLE trials. Chin Clin Oncol 4(3):33, 9/2015. PMID: 26408300.
- Halperin DM, Lee JJ, Dagohoy CG, Yao JC. Rational Clinical Experiment: Assessing Prior Probability and Its Impact on the Success of Phase II Clinical Trials. J Clin Oncol 33(26):2914-9, 9/2015. e-Pub 8/2015. PMCID: PMC4554752.
- Lee JJ. Commentary on Hey and Kimmelman. Clin Trials 12(2):110-2, 4/2015. e-Pub 2/2015. PMCID: PMC4492278.
- Hobbs BP, Chen N, Lee JJ. Controlled multi-arm platform design using predictive probability. Stat Methods Med Res. e-Pub 1/2016. PMCID: PMC5039108.
- Gu X, Chen N, Wei C, Liu S, Papadimitrakopoulou VA, Herbst RS, Lee JJ . Bayesian Two-Stage Biomarker-Based Adaptive Design for Targeted Therapy Development. Stat Biosci 8((1)):99-128, 6/2016. e-Pub 12/2014. PMCID: PMC5014437.
- Zang Y, Lee JJ. A robust two-stage design identifying the optimal biological dose for phase I/II clinical trials. Stat Med 36(1):27-42, 1/2017. e-Pub 8/2016. PMCID: PMC5138134.
- Du Y, Cook JD, Lee JJ. Comparing three regularization methods to avoid extreme allocation probability in response-adaptive randomization. J Biopharm Stat:1-11. e-Pub 2/2017. PMID: 28323532.
- Kim S, Baladandayuthapani V, Lee JJ. Prediction-Oriented Marker Selection (PROMISE): With Application to High-Dimensional Regression. Stat Biosci 9(1):217-245, 6/2017. e-Pub 9/2016. PMCID: PMC5543994.
- Jiang F, Ma Y, Lee, JJ. A second-order semiparametric method for survival analysis, with application to an acquired immune deficiency syndrome clinical trial study. Journal of the Royal Statistical Society Series C: Applied Statistics 66(4):833-846, 2017.
- Yin G, Chen N, Lee JJ. Bayesian Adaptive Randomization and Trial Monitoring with Predictive Probability for Time-to-Event Endpoint. Statistics in Biosciences:1-19, 2017.
-
Missing Data Analysis
- Ahn, J.*, Liu, S., Wang W. and Yuan, Y. (2013) Bayesian Latent-class Mixed-effect Hybrid Models for Dyadic Longitudinal Data with Non-ignorable Dropouts. Biometrics, 69, 914-924.
- Zhang G. and Yuan, Y. (2012) Modeling Longitudinal Dyadic Data with Nonignorable Dropout with Application to a Breast Cancer Study. Annals of Applied Statistics, 6, 753-771.
- Yuan, Y. and Yin, G. (2010). Quantile regression for longitudinal studies with nonignorable missing data. Biometrics, 66, 105-114.
- Yuan, Y. and Little, R.J.A. (2009) Meta-analysis of studies with missing data. Biometrics 65, 487-496.
- Yuan, Y. and Little, R.J.A. (2009) Mixed-effect hybrid models for longitudinal data with nonignorable dropout. Biometrics 65, 478-486. Yuan, Y., and Little, R.J.A. (2007) Model-Based Estimates of the Finite Population Mean for Two-Stage Cluster Samples with Unit Non-response. Journal of the Royal Statistical Society: Series C 56, 79-97.
- Yuan, Y., and Little, R.J.A. (2007) Parametric and Semiparametric Model-based Estimates of the Finite Population Mean for Two-Stage Cluster Samples with Item Nonresponse. Biometrics 63, 1172-1180.
-
Mediation Analysis
- Huang, J.* and Yuan, Y. (2016) Bayesian Dynamic Mediation Analysis, Psychological Methods, to appear.
- Yuan, Y. and MacKinnon D. (2014) Robust mediation analysis based on mediation regression. Psychological Methods, 19, 1-20.
- Yuan, Y. and MacKinnon D. (2009) Bayesian mediation analysis. Psychological Methods, 14, 301-322.
~69,000 USERS WORLDWIDE
SOME OF OUR USERS


Get In Touch
Welcome to the Trial Design website
If this is your first visit, please create a user account. Returning users should select the appropriate option below.